本帖最后由 sunsong7 于 2015-1-6 10:44 编辑 6 b8 v- h" v$ N" z
' m+ g W) m: c 概要:埃博拉病毒急性感染具有极高的致死率,其基本特征表现在机体的先天免疫与过继免疫反应被压制,病毒疯狂复制引发强烈的细胞因子风暴并攻击血管系统,大面积细胞凋亡导致脓血症和多脏器功能衰竭,病人最终因体温下降、血压过低休克致死。在缺乏特异性治疗药物干预的情况下,仍有一部分感染者会自然康复,说明埃博拉感染是一种自限性疾病,机体自身的免疫系统在非特异性治疗措施帮助下最终能够清除病毒。埃博拉病毒部分地阻断了I型干扰素的产生和抗病毒信号途径,但有证据表明I型干扰素仍能够在一定程度上抑制病毒复制,潜伏期内予以预防性注射I型干扰素可望大幅度降低感染者体内病毒负载;间充质干细胞具有强大及可塑性的免疫调节作用,能够压制细胞因子风暴,支持血管内皮细胞增殖,抑制细胞凋亡,具有向炎症组织趋化和参与修复的能力,对于埃博拉感染终末期患者采用间充质干细胞治疗有望显著降低死亡风险和后遗症的发生率。当前绝大多数常见的病毒性感染缺乏特异性治疗药物,在相当长一段时期内,非特异性治疗手段仍是对抗病毒性疾病的基本策略。$ a/ g% I6 H0 M. r6 ~; ]$ }2 P$ u9 z% Y6 o( L
! x- ~# @+ G2 U- W* A# b' E& g& i! C
* X0 N6 L3 B5 L
" m7 E+ u r! g$ _. c
@, ^ i) C* H* UAgainst Ebola: type I interferon guard risk and mesenchymal stromal cell combat sepsis
( R1 y9 y: i0 |! L
3 N2 J* S) I* H- s5 P9 V & G) ~- `: k a: x2 ]* J5 R
" B! ^9 _; D! O, [
. G; ~4 y8 h* Z3 W The 2014 Ebola outbreak in West Africa triggered a global crisis. Nine countries havereported more than 20000 infection cases in total and nearly 8000 lives have been lost. The actual death toll is likely much higher than this figure; the death rate is as high as 70%, consideringconfirmed cases.' R' j- r- g: n" d+ N
The Ebola virus launches its destruction by shutting down the host’s innate and adaptiveimmune systems. The virus then replicates itself out of control and causes a cytokine storm in the host. Consequently, the host’s overdriven immune system attacks its own endothelial cells and this leads to multiple organ hemorrhagic damage, the host dies of septic shock finally. Under current circumstances where no specific interventions have shown effectivenessagainst the virus, our opinions are justified in applying a non-specific anti-viral approachduring the incubation period of virus infection as an essential protection to put the host’s immune system into an alert state and henceforth to slow down the viral replication. When the viral infection proceeds to the terminal stage, the key factor would be applying a non-specific immune modulationapproach to suppress the cytokine storm that causes multiple organ failure, in an attempt to open a time window for the host’s immune system to recover.
7 o( x7 Q# k, W4 x/ A. y. _
; `( K% C! ^5 f+ N! f! t- H
2 I8 `0 ^/ {- ?* Q" n% |: S' BWhat makes the Ebola infection so deadly?7 X, @7 h' l7 B. I- ^+ W3 q
# j" h) ^2 m0 M% B( p7 `' h
7 q* v) |3 p& P4 [4 y1 j. x& u! kThe Ebola virus invades antigen presenting cells (APCs) quietly and turns their alarm system off essentially, so that the immune system remains inactivated toward the virus. The virus then growsuncontrollably and invades many organs. Eventually, many premature cells start dying and exploding, and these cells release all their contents, including signal molecules, into the blood. The signals eventually trigger the extreme immune attacks, which cause arteries, veins and capillaries to leak blood and plasma. The host’s body temperature drops and blood pressure falls,causing the host to go into a severe septic shock.4 v% G# v* j+ I% O, Y1 D6 x
+ f8 [3 t, m/ f! XThe infection of the Ebola virus; The impairment of innate and adaptive immunity;
4 H) r) E: @& @: I' _; b The severe attacks of dysregulated immune system;
, X/ Q6 ^6 ], W8 B% r Diffusive bleeding and hypotensive shock eventually kill the patients.
' G& Z% C5 { j6 x . g! H- ^5 s9 k( x6 [
1 S3 o5 Y+ O) m8 n
: D# S+ o0 c, F" e

, u3 F0 o' F% z$ { x( ~. A
1 C. T9 @$ x; S8 I6 I" x) w
1 J: \( L) i& r+ u5 w9 \5 f9 G6 OFig. 1 System overview of Ebola pathogenesis
. l7 }' T2 F/ D
( M$ S% q; k* W5 x+ a( T5 N6 L4 Q9 i+ m, h( N
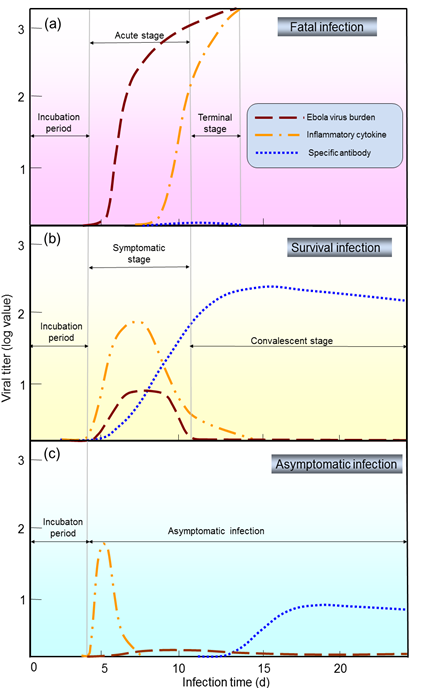
What are the differences among fatal, survival and symptomless infection?; N w* J0 [+ F0 W9 U# n
7 b0 ]4 L" I0 U7 k+ h; G+ P" K Ebola infection is generally composed of the incubation period, the symptomatic/acute stage, and the convalescent/terminal stage. The virus burden, inflammatory response, and specific antibodies are the main contributors to different outcomes: mortality, survival, or symptomless infection (Fig. 2), suggesting that the appropriate intervention strategy in each stage would accordingly be able to control the Ebola virus.4 A2 T: H S3 ~5 G/ W" \+ |& i
* i) t# x1 C+ Q# O6 M# b( ~6 N# b5 S ]$ B
, h( J! i7 b- c/ P8 S3 P$ r9 y
& Q; o9 |5 O; FFig. 2 Abridged general view of different profiles of immune responses in fatal (a), survival (b), and asymptomatic (c) Ebola infections
3 M8 X1 Q! ~, W
7 Z% F, c) g. z& p" E7 L# \& ?5 R7 d, _! Z+ F7 \ } M. }
The double edges of inflammatory response; The distinction of specific antibodies; The diversity of the virus burden; The depletion of relevant cells; Some patients indeed recovered from the Ebola infection without receiving specific interventions; Appropriate immune responses can help the body heal itself. " g6 }/ E, p' B* ]
; j8 k3 W) M' f: R4 w
A prospective strategy
( t. U; }5 W8 E2 C% S5 v8 r4 D& S) j
In the symptomatic stage, the supportive care is mainly toward aggressive prevention of intravascular volume depletion, correction of profound electrolyte abnormalities, and prevention of the shock complications. There is neither precaution for the incubation period nor effective medication for the terminal stage. We propose that a preventative antiviral intervention for the incubation period may lower the consequent virus burden. Furthermore, we propose that an immunomodulatory strategy for the terminal stage may reduce the damages caused by the cytokine storm, thus prolonging the survival time of the patients, making it possible for the patients’ adoptive immunity to recover and beat the infection.
M. P9 o% f" R$ E2 h; ?) p' V8 m$ ^7 uType I IFN intervention during the incubation period may render a beneficial outcome( [8 B* _; D9 x* g' B% n& u% B
9 |' e4 }& Z7 F
8 Z3 Q4 F! z, {5 A. \
, s) Y: ~6 Y0 i' ?9 Y. X& }Fig. 3 Type I IFN controls innate and adaptive immunity and intracellular antiviral programs
$ G& T+ P( T) Y. T; H
" n5 p9 [) q, I# j+ V6 s) W( xType I interferons have a broad spectrum of antiviral capability that are able to fight most virus infections; Recombinant IFN-α2b (200 IU/ml) can suppressed Ebola replication by 100-folds in Vero cells in vitro; Early treatment on Ebola-infected cynomolgus with recombinant IFN-α2b delayed onset of viremia and death by several days; IFN-β treatment was associated with reducing the plasma and tissue viral burden, significantly increased survival time in Ebola infected macaques in vivo; Exogenous administration of type I interferon may induce uninfected cells into an antiviral state. Type I interferon might limit the spread of the Ebola virus and prolong survival if administered immediately after exposure to Ebola viruses. ) D# M& J* U( M3 Y
Mesenchymal stromal cell therapy during the terminal stage may prevent cytokine storm, massive cell apoptosis, and septic shock
5 c4 @0 J% ?( y: f$ y, p/ T& {% m. X: h
/ a9 c# d0 a4 J S; d9 o
! ^% @+ q8 j2 s v V& ]9 L5 _
. l! l/ T' ?9 I# i7 ]& l# U& eFig. 4 Immunological function of MSCs on different cell types of the innate/adaptive immunosystem while MSCs diminish damage and induce repair
& |) F w5 |& k$ g
1 q( B2 Z+ i) Z1 K1 a( E
" x) J. L d/ m1 d. {4 G1 w; d% c8 F5 j' I' ]7 Y' g
The significant differences in fatality rate between age groups may be relavent to the consumption of age-related changes in the stem cells reservoir; MSCs migrate to injured tissue sites where they can inhibit the release of pro-inflammatory cytokines and promote the survival of damaged cells; MSCs operate through a variety of effector mechanisms on key cells of the innate and adaptive immune systems; MSCs can specifically communicate with the inflammatory microenvironment and this immunoregulatory function of MSCs is highly plastic ; It would be interesting to use the available nonhuman primate models of EVD to test such a therapeutic hypothesis.
4 q* L3 S9 ]& ]
Non-specific treatment as an essential strategy against viral diseases in the foreseeable future
) [+ r1 u; b* x8 F rIt has been almost forty years since the first Ebola outbreak in 1976. There has been no specific therapy for even the most common human viral infection,the outlook for the development of Ebola therapeutics is not optimistic. In the symptomatic stage, the supportive care is mainly toward aggressive prevention; There is neither precaution for the incubation period nor effective medications for the terminal stage; A preventative antiviral intervention for the incubation period may lower the consequent virus burden; An immunomodulatory strategy for the terminal stage may reduce the damages caused by the cytokine storm, thus prolong the survival time of the patients; When our immune system is given sufficient time for intentionally activation when we are exposed to deadly viruses, there is a good chance that it can gear up and eliminate the viruses by itself.- \$ }' K7 G& H2 _
( k7 c; b4 S i" m
4 G' j8 ?( T! S C6 n" ^: w【原文下载】http://www.zju.edu.cn/jzus/article.php?doi=10.1631/jzus.B1400365
( G1 [$ [) A- m/ E% F$ G( Z: a: N1 i h: a9 @
% T7 X8 K" d- D A% g
|


















 发表于 2015-1-6 10:02
发表于 2015-1-6 10:02
